Theory
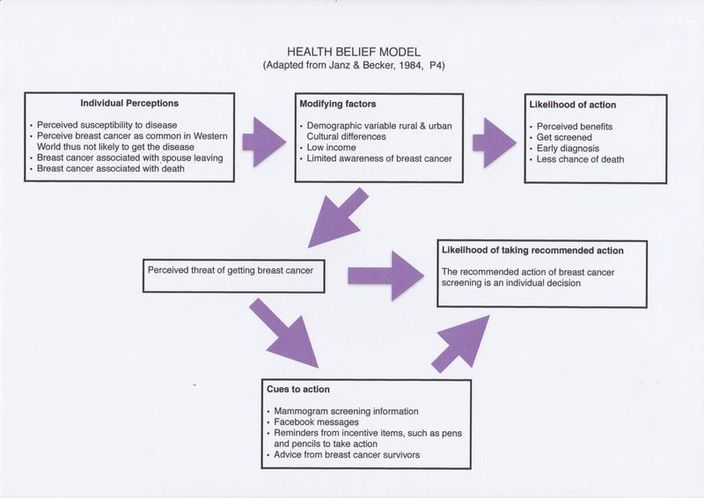
The theoretical framework used in breast cancer awareness among Kenyan women is referred to as the Health Belief Model (HBM) (13). The HBM is a behavioural health theory used in health promotion, which is a combination of knowledge, opinion and actions taken by an individual or group in reference to their health.
Han et al (2009) recommend the importance of using theory based tailored approaches as they are more than likely to enhance screening interventions leading to early detection (10). Developed in 1950 by a social psychologist of the United States Public Health, the HBM has since been revised (6 &13).
The HBM has been specifically used to identify interventions that address perceived barriers and benefits. According to the HBM, the perceiver will eventually decide what he or she wants to do in accordance with his or her belief system. The choice to take action is placed on the individual (4).
This particular theory is interpersonal, meaning it’s based on knowledge and beliefs of each individual person. The HBM is used to develop preventative health programmes, as well as design appropriate intervention programmes where prevention has failed.
The HBM consists of the following dimensions: (a) perceived susceptibility, (b) perceived severity, (c) perceived barriers and (d) perceived benefits. If individuals are aware that they may get a disease or condition, then they are more likely to take the necessary action to prevent the disease from occurring, if they perceive that the benefits they would get from the behaviour are beneficial to them (13).
Perceived susceptibility, when a person recognises a reason to be concerned about a particular disease. For example breast cancer is dangerous.
Perceived severity, when a person realises that they may be personally vulnerable to this particular disease. Portray the seriousness of the disease and severe consequences of not taking action. Being overweight or obese is known to place an individual at a higher risk of developing breast cancer. However, if an individual doesn't feel they are at risk of developing breast cancer, based on the fact that they have never had any symptoms, then they will be less likely to change their behaviour .
Perceived benefits, when a person weighs the positive outcomes that can occur from behaviour they will be more likely to change their behaviour. A person must determine that changing their behaviour will improve their health, but this needs to be achieved within their means. If a person decides that breast cancer is a notable health concern, and that they are personally vulnerable to this disease process, then they may be willing to change their behaviour and engage in preventive measures.
Perceived barriers, if a person determines that the barriers to changing their behaviours are greater than the possible benefits, they will not follow through. Barriers could include cost associated with the health behaviour change, negative outcomes of the disease (fear of death if diagnosed with breast cancer, losing part of the body) and lack of family support. The pros (benefits) have to outweigh the cons (barriers).
Cues to action, provide information and incentive items containing visual reminders or recommended action.
Self-Efficacy, build people's confidence that they can successfully complete this behaviour change by giving them tools to reduce anxiety about the change.
Strengths and Limitations of HBM
One strength of using the HBM for this piece of work is the possibility of increasing awareness among Kenyan women about the recommended use of mammogram screening. Increasing awareness can act as a catalyst for changes in behaviour, thereby increasing rates of mammogram screening. Another strength is that HBM focuses on health promotion. There is substantial evidence that supports the idea that spousal involvement increases mammogram screening. This may either increase uptake or decrease it, depending on whether the spouses perceive benefits associated with their wives undergoing mammograms. Spousal involvement may also serve as a cue for the women to get the mammogram screening.
Lack of mammogram screening among Kenyan women is very prevalent. This lack of preventative medicine use is partly linked to their beliefs and culture (15). A limitation of applying the HBM to this group is that at certain times it may be difficult to alter an individual’s perception because of lack of adequate time to receive education. Another limitation may be due to fears among the Kenyan women when it comes to seeking healthcare. This fear is often due to the perceived seriousness of what may occur if diagnosed with the disease, including fear of death, spouse leaving, losing a breast through mastectomy, etc (9). It is also important to recognise that some health behaviours may not be cultural, but rather are personal habits that may create additional barriers for women when it comes to seeking mammogram screenings. Finally, there is no evidence that the HBM has been applied to situations involving Kenyan women; therefore its applicability to this population has been assumed. Because the HBM is a cognitively based model, when it comes to cultural factors, it is limited regarding consideration for such (6 & 13).
Han et al (2009) recommend the importance of using theory based tailored approaches as they are more than likely to enhance screening interventions leading to early detection (10). Developed in 1950 by a social psychologist of the United States Public Health, the HBM has since been revised (6 &13).
The HBM has been specifically used to identify interventions that address perceived barriers and benefits. According to the HBM, the perceiver will eventually decide what he or she wants to do in accordance with his or her belief system. The choice to take action is placed on the individual (4).
This particular theory is interpersonal, meaning it’s based on knowledge and beliefs of each individual person. The HBM is used to develop preventative health programmes, as well as design appropriate intervention programmes where prevention has failed.
The HBM consists of the following dimensions: (a) perceived susceptibility, (b) perceived severity, (c) perceived barriers and (d) perceived benefits. If individuals are aware that they may get a disease or condition, then they are more likely to take the necessary action to prevent the disease from occurring, if they perceive that the benefits they would get from the behaviour are beneficial to them (13).
Perceived susceptibility, when a person recognises a reason to be concerned about a particular disease. For example breast cancer is dangerous.
Perceived severity, when a person realises that they may be personally vulnerable to this particular disease. Portray the seriousness of the disease and severe consequences of not taking action. Being overweight or obese is known to place an individual at a higher risk of developing breast cancer. However, if an individual doesn't feel they are at risk of developing breast cancer, based on the fact that they have never had any symptoms, then they will be less likely to change their behaviour .
Perceived benefits, when a person weighs the positive outcomes that can occur from behaviour they will be more likely to change their behaviour. A person must determine that changing their behaviour will improve their health, but this needs to be achieved within their means. If a person decides that breast cancer is a notable health concern, and that they are personally vulnerable to this disease process, then they may be willing to change their behaviour and engage in preventive measures.
Perceived barriers, if a person determines that the barriers to changing their behaviours are greater than the possible benefits, they will not follow through. Barriers could include cost associated with the health behaviour change, negative outcomes of the disease (fear of death if diagnosed with breast cancer, losing part of the body) and lack of family support. The pros (benefits) have to outweigh the cons (barriers).
Cues to action, provide information and incentive items containing visual reminders or recommended action.
Self-Efficacy, build people's confidence that they can successfully complete this behaviour change by giving them tools to reduce anxiety about the change.
Strengths and Limitations of HBM
One strength of using the HBM for this piece of work is the possibility of increasing awareness among Kenyan women about the recommended use of mammogram screening. Increasing awareness can act as a catalyst for changes in behaviour, thereby increasing rates of mammogram screening. Another strength is that HBM focuses on health promotion. There is substantial evidence that supports the idea that spousal involvement increases mammogram screening. This may either increase uptake or decrease it, depending on whether the spouses perceive benefits associated with their wives undergoing mammograms. Spousal involvement may also serve as a cue for the women to get the mammogram screening.
Lack of mammogram screening among Kenyan women is very prevalent. This lack of preventative medicine use is partly linked to their beliefs and culture (15). A limitation of applying the HBM to this group is that at certain times it may be difficult to alter an individual’s perception because of lack of adequate time to receive education. Another limitation may be due to fears among the Kenyan women when it comes to seeking healthcare. This fear is often due to the perceived seriousness of what may occur if diagnosed with the disease, including fear of death, spouse leaving, losing a breast through mastectomy, etc (9). It is also important to recognise that some health behaviours may not be cultural, but rather are personal habits that may create additional barriers for women when it comes to seeking mammogram screenings. Finally, there is no evidence that the HBM has been applied to situations involving Kenyan women; therefore its applicability to this population has been assumed. Because the HBM is a cognitively based model, when it comes to cultural factors, it is limited regarding consideration for such (6 & 13).
